Catheter Tip & PIVC Position
TERMINOLOGY
Common language facilitates communication between professional and organisations, the translation of evidence into clinical practice, data sharing, and research. CNSA, eviQ and eviQ Education are leading vascular access management and education in cancer care in Australia utilizing common, contemporary terminology (Table 1).
Table 1: CVAD terminology
INTRODUCTION
The catheter tip of a Central Venous Access Device (CVAD) is the internal or distal end of the catheter. There is much discussion in the literature about the optimal position of the CVAD catheter tip and the relationship between catheter tip position and functional complications such as occlusion (1). This question will discuss current evidence for the optimal catheter tip location, the methods of determining the catheter tip location and complications associated with tip malposition.
The majority of studies noting catheter tip position were observational or incidental findings in retrospective studies which primarily documented incidence rates of CVAD complications. It is unlikely that high quality studies, for example randomised controlled trials comparing the recommended or ideal catheter tip position versus suboptimal position will be undertaken because it would be unethical with documented detimental effects of catheter tip malposition. Hence, recommendations included in this answer will be supported by other literature, for example international recommendations and standards of practice.
Literature that discussed the optimal insertion site of Peripheral Intravenous Cannulas (PIVCs) to reduce the risk of complications, identified in this review of the cancer patient cohort, was expert opinion. Therefore, literature for all patient cohorts was used to support the practice recommendations.
SUMMARY OF RECOMMENDATIONS
CENTRAL VENOUS ACCESS DEVICES:
CNSA recommends for adult and paediatric patients with cancer:
-
Optimal catheter tip position of Central Venous Access Devices is at the cavoatrial junction (1-11), and in acceptable position of the lower third of the superior vena cava (3,12-21) and the upper right atrium (3,14,22-24).
-
Technique of identifying the catheter tip location: can be determined by
-
use of intracavity electrocardiographic (ECG) guidance during the insertion procedure (1,15,25,26)
-
radiological examination including:
-
chest x-ray immediately post procedure and prior to first use (2,6,10,13,20,21,23,27-31) and investigation of complications e.g. malposition, catheter migration, kinking, pinch-off syndrome (32) and with arms beside the body (33)
-
avoid fluoroscopy due to patient exposure to ionizing radiation (34)
-
-
PERIPHERAL INTRAVENOUS CANNULA (PIVC)
CNSA recommends the optimal peripheral intravenous cannula insertion site to reduce the risk of all complications for adults are the veins in the forearm including the metacarpal, cephalic, basilic, and median veins, and the veins in the hand, forearm, and foot if not walking for paediatrics (35) and:
Adult patients:
-
Avoid areas of flexion (including antecubital fossa and wrist), pain, impaired skin, infection (in same limb), lower limbs, and superficial veins on the torso
-
Consider veins on hand for short-term use e.g less than 24 hours
-
Avoid insertion sites distal to recent venepuncture or insertion sites to reduce the risk of extravasation (32)
Paediatric patients:
-
Avoid antecubital fossa
SECTION A: CENTRAL VENOUS ACCESS DEVICES
1. OPTIMAL CATHETER TIP - CVAD
1.1 Summary of Evidence
Numerous adult and paediatric studies state the optimal position for the CVAD catheter tip is within a defined range between the lower third of the superior vena cava, cavoatrial junction to the upper right atrium (14,21,22,30,36). A small number of adult and paediatric studies state the superior vena cava is acceptable (29,31,37,38). However, a larger number of studies specify the optimal catheter tip position is the lower third of the superior vena cava (3,12-22). Optimal catheter tip at the cavoatrial junction (CAJ) is supported by numerous adult and paediatric studies (1-11,15). The cavoatrial junction (CAJ) is where the right lateral border of the superior vena cava (SVC) meets the superior border of the right atrium (39). A smaller number of studies identify the upper right atrium is also an acceptable catheter tip position (3,14,22-24). The optimal catheter tip position is an observational finding in these retrospective studies which primarily documented incidence rates of CVAD complications.
One study of femorally inserted central catheters (FICCs) stated a catheter tip position in the inferior vena cava between the third and fourth lumbar vertebra on imaging was acceptable (40).
1.2 Practice Recommendation
CNSA recommends the optimal catheter tip position of Central Venous Access Devices for adult and paediatric patients with cancer is at the cavoatrial junction (1-11), and in acceptable position of the lower third of the superior vena cava (3,12-21) and the upper right atrium (3,14,22-24).
GRADE: A/P
1.3 Visual Representation
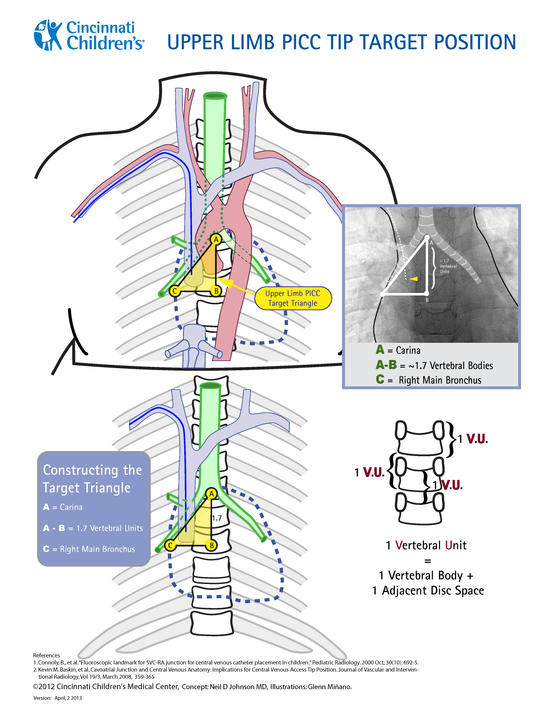
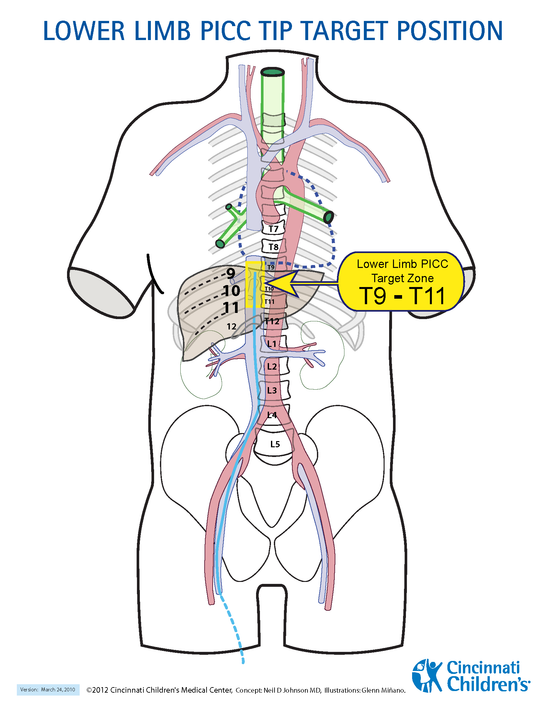
The lower third of the superior vena cava, cavoatrial junction to the upper right atrium is highlighted in yellow in the diagram:
|
|
|
Figure 1: upper limb PICC tip placement |
Figure 2: lower limb PICC tip placement |
|
Illustrations: ©2020 Cincinnati Children's Medical Center, Concept: Neil D Johnson MD, Illustrations: Glenn Miñano http://stopivharm.org/ |
|

Chest x-ray:
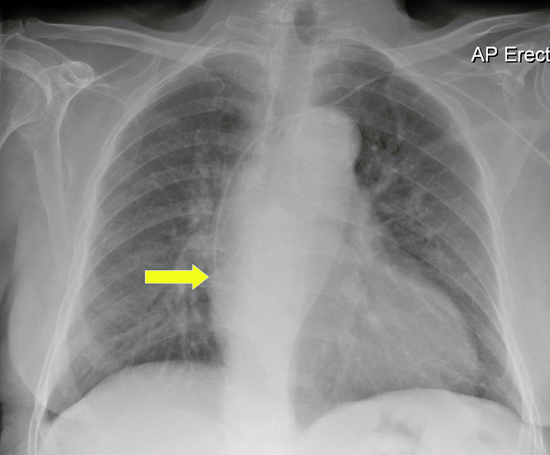

Figure 3: Chest x-ray with catheter tip at cavoatrial junction
Intracavity ECG
Use of new technology or catheter guidewire or column of sodium chloride connected to a ECG monitor to identify when the p wave is peaked which indicates when the catheter tip is at the cavoatrial junction:

2. TECHNIQUE OF IDENTIFYING THE CATHETER TIP LOCATION
2.1 Summary of Evidence
Location of the catheter tip can be performed during or after the insertion procedure.
During the procedure:
- Intracavity electrocardiograph (IC-ECG) guidance utilizes the ECG wave form to establish the location of the cavoatrial junction (1,15,25 26)
- Radiological examination: a number of studies describe using intraprocedure CXR or fluoroscopy (5,7), fluoroscopy (7,9,18,42,43), or fluoroscopy or ECG guidance (3,12). One study used angiographic examination after the injection of contrast media (36).
Post procedure:
-
Studies identified using chest x-ray (CXR) or fluoroscopy (11,16). The majority of studies described the use of CXRs performed after the procedure and prior to CVAD use for the first time (2,6,10,13,20,21,23,27-31,44).
2.2 Practice Recommendation
CNSA recommends the catheter tip position of Central Venous Access Devices for adult and paediatric patients with cancer can be determined by:
-
real-time use of intracavity electrocardiograph guidance during the insertion procedure (1,15,25,26)
-
or radiological examination including:
-
e.g., chest x-ray immediately post procedure and prior to first use (2,6,10,13,20,21,23,27-31) and investigation of complications e.g. malposition, catheter migration, kinking, pinch-off syndrome (32)
-
with arms beside the body (33)
-
avoid fluoroscopy due to patient exposure to ionizing radiation (34)
-
GRADE: V
3. IMPACT OF CATHETER TIP POSITION
Catheter tips not located at the cavoatrial junction are associated with a higher risk of complications including (1) functional complications (1) including occlusions (11,21,26) which are associated with (2) deep vein thrombosis (22,34,45).
1. Functional complications:
- Catheter tip in the superior vena cava compared to right atrium had an increased risk of occlusion by 2.7 times in a paediatric, prospective data registry (42)
- 80.6% of malfunctions were associated with tip malposition in a descriptive, retrospective study (15)
- Irreversible complete occlusions were 22 times more likely to occur with catheter malposition, that is out of the lower third of the superior vena cava in an observational cohort study (13)
- Suboptimal catheter tip position was identified to be a statistically significant risk factor for occlusion and premature TIVAD removal in a cohort study of 235 adult participants with TIVADs (21)
- Higher risk of malfunction with catheter tip malposition in a consensus statement by international vascular access experts (36)
- High risk profile for development of peripheral and central venous access device occlusions (19)
2. Thrombosis:
- A significant risk of thrombosis with catheter tip malpositon was noted in a retrospective cohort study of 488 paediatric participants identified (46)
- A reduced risk of thrombosis and fibrin sleeve formation at the catheter tip when in the correct position was noted in a questionnaire of adult and paediatric oncology centres (22).
- Catheter tip malposition is a major risk of CVAD related DVTs in expert opinion article (17)
In contrast, 93% patients had no complications when the catheter tip was located in the recommended lower superior vena cava and at the cavoatrial junction in a prospective cohort study in 477 adult participants (30). Low numbers of thrombotic complications were related to accurate positioning of the catheter tip at the cavoatrial junction in a retrospective study of 1247 adults (5).
SECTION B: PERIPHERAL INTRAVENOUS CANNULA (PIVC)
4. OPTIMAL SITE
4.1 Summary of Evidence
There are three expert opinion articles that briefly discuss Peripheral Intravenous Cannulas. Therefore practice recommendations in the following section are supported by evidence not specific to patients with cancer therefore literature was sought from outside of cancer care.
4.2 Practice Recommendation
CNSA recommends the optimal peripheral intravenous cannula insertion site to reduce the risk of all complications for adults are the veins in the forearm including the metacarpal, cephalic, basilic, and median veins, and the veins in the hand, forearm, and foot if not walking for paediatrics (35) and:
Adult patients:
-
Avoid areas of flexion (including cubital fossa and wrist), pain, impaired skin, infection (in same limb), lower limbs, and superficial veins on the torso
-
Consider veins on hand for short-term use e.g less than 24 hours
-
Avoid insertion sites distal to recent venepuncture or insertion sites to reduce the risk of extravasation (32)
Paediatric patients:
-
Avoid antecubital fossa (35)
GRADE: Committee Consensus
REFERENCES
1. Goossens GA, Jerome M, Janssens C, Peetermans WE, Fieuws S, Moons P, et al. Comparing normal saline versus diluted heparin to lock non-valved totally implantable venous access devices in cancer patients: a randomised, non-inferiority, open trial. Ann Oncol. 2013;24(7):1892-9.
2. Bellesi S, Chiusolo P, De Pascale G, Pittiruti M, Scoppettuolo G, Metafuni E, et al. Peripherally inserted central catheters (PICCs) in the management of oncohematological patients submitted to autologous stem cell transplantation. Supportive Care in Cancer. 2013;21(2):531-5.
3. Chopra V, Flanders SA, Saint S, Woller SC, O'Grady NP, Safdar N, et al. The Michigan Appropriateness Guide for Intravenous Catheters (MAGIC): Results From a Multispecialty Panel Using the RAND/UCLA Appropriateness Method. Ann Intern Med. 2015;163(6 Suppl):S1-40.
4. Giordano P, Saracco P, Grassi M, Luciani M, Banov L, Carraro F, et al. Recommendations for the use of long-term central venous catheter (CVC) in children with hemato-oncological disorders: management of CVC-related occlusion and CVC-related thrombosis. On behalf of the coagulation defects working group and the supportive therapy working group of the Italian Association of Pediatric Hematology and Oncology (AIEOP). Ann Hematol. 2015;94(11):1765-76.
5. Jan HC, Chou SJ, Chen TH, Lee CI, Chen TK, Lou MA. Management and prevention of complications of subcutaneous intravenous infusion port. Surg Oncol. 2012;21(1):7-13.
6. Nam SH, Kim DY, Kim SC, Kim IK. Complications and risk factors of infection in pediatric hemato-oncology patients with totally implantable access ports (TIAPs). Pediatric Blood & Cancer. 2010;54(4):546-51.
7. Paquet F, Boucher LM, Valenti D, Lindsay R. Impact of arm selection on the incidence of PICC complications: results of a randomized controlled trial. J. 2017;18(5):408‐14.
8. Schulmeister L. Management of non-infectious central venous access device complications. Seminars in Oncology Nursing. 2010;26(2):132-41.
9. Teichgraber UK, Kausche S, Nagel SN. Evaluation of radiologically implanted central venous port systems explanted due to complications. J. 2011;12(4):306-12.
10. Wu CY, Hu HC, Ko PJ, Fu JY, Wu CF, Liu YH, et al. Risk factors and possible mechanisms of superior vena cava intravenous port malfunction. Ann Surg. 2012;255(5):971-5.
11. Zaghal A, Khalife M, Mukherji D, El Majzoub N, Shamseddine A, Hoballah J, et al. Update on totally implantable venous access devices. Surg Oncol. 2012;21(3):207-15.
12. Bertoglio S, Faccini B, Lalli L, Cafiero F, Bruzzi P. Peripherally inserted central catheters (PICCs) in cancer patients under chemotherapy: A prospective study on the incidence of complications and overall failures. J Surg Oncol. 2016.
13. Bertoglio S, Solari N, Meszaros P, Vassallo F, Bonvento M, Pastorino S, et al. Efficacy of normal saline versus heparinized saline solution for locking catheters of totally implantable long-term central vascular access devices in adult cancer patients. Cancer Nursing. 2012;35(4):E35-42.
14. Dal Molin A, Clerico M, Baccini M, Guerretta L, Sartorello B, Rasero L. Normal saline versus heparin solution to lock totally implanted venous access devices: Results from a multicenter randomized trial. European Journal of Oncology Nursing. 2015;19(6):638-43.
15. Goossens GA, Stas M, Moons P. Management of functional complications of totally implantable venous access devices by an advanced practice nursing team: 5 years of clinical experience. European Journal of Oncology Nursing. 2012;16(5):465-71.
16. Hitchcock J. Preventing intraluminal occlusion in peripherally inserted central catheters. British Journal of Nursing. 2016;25(19):S12-S8.
17. Linnemann B. Management of complications related to central venous catheters in cancer patients: an update. Seminars in Thrombosis & Hemostasis. 2014;40(3):382-94.
18. Lo Priore E, Fliedner M, Heverhagen JT, Novak U, Marschall J. The role of a surveillance programme for intro-ducing peripherally inserted central catheters: a 2-year observational study in an academic hospital. Swiss Med Wkly. 2017;147:w14441.
19. Matey L, Camp-Sorrell D. Venous Access Devices: Clinical Rounds. Asia-Pac. 2016;3(4):357-64.
20. Palese A, Baldassar D, Rupil A, Bonanni G, Capellari Maria T, Contessi D, et al. Maintaining patency in totally implantable venous access devices (TIVAD): a time-to-event analysis of different lock irrigation intervals. European Journal of Oncology Nursing. 2014;18(1):66-71.
21. Wang YC, Lin PL, Chou WH, Lin CP, Huang CH. Long-term outcomes of totally implantable venous access devices. Supportive Care in Cancer. 2017;25(February 9th).
22. Dal Molin A, Guerretta L, Mazzufero F, Rasero L. The management of totally implanted venous ports in the ambulatory oncologic patient. J. 2009;10(1):22-6.
23. Granic M, Zdravkovic D, Krstajic S, Kostic S, Simic A, Sarac M, et al. Totally implantable central venous catheters of the port-acath type: complications due to its use in the treatment of cancer patients. J. 2014;19(3):842-6.
24. Odabas H, Ozdemir NY, Ziraman I, Aksoy S, Abali H, Oksuzoglu B, et al. Effect of port-care frequency on venous port catheter-related complications in cancer patients. Int J Clin Oncol. 2014;19(4):761-6.
25. Goossens GA, De Waele Y, Jérôme M, Fieuws S, Janssens C, Stas M, et al. Diagnostic accuracy of the Catheter Injection and Aspiration (CINAS) classification for assessing the function of totally implantable venous access devices. Supportive Care in Cancer. 2016(July 26th).
26. Schiffer CA, Mangu PB, Wade JC, Camp-Sorrell D, Cope DG, El-Rayes BF, et al. Central venous catheter care for the patient with cancer: American Society of Clinical Oncology clinical practice guideline. Journal of Clinical Oncology. 2013;31(10):1357-70.
27. Borretta L, MacDonald T, Digout C, Smith N, Fernandez CV, Kulkarni K. Peripherally Inserted Central Catheters in Pediatric Oncology Patients: A 15-Year Population-based Review From Maritimes, Canada. J Pediatr Hematol Oncol. 2018;40(1):e55-e60.
28. Garajova I, Nepoti G, Paragona M, Brandi G, Biasco G. Port-a-Cath-related complications in 252 patients with solid tissue tumours and the first report of heparin-induced delayed hypersensitivity after Port-a-Cath heparinisation. European Journal of Cancer Care. 2013;22(1):125-32.
29. Heibl C, Trommet V, Burgstaller S, Mayrbaeurl B, Baldinger C, Koplmuller R, et al. Complications associated with the use of Port-a-Caths in patients with malignant or haematological disease: a single-centre prospective analysis. European Journal of Cancer Care. 2010;19(5):676-81.
30. Kang J, Chen W, Sun W, Ge R, Li H, Ma E, et al. Peripherally inserted central catheter-related complications in cancer patients: a prospective study of over 50,000 catheter days. The Journal of Vascular Access. 2017;18(2):153-7.
31. Lin S, Wen K, Liu C, Wei C. The Use of Peripherally Inserted Central Catheters in Cancer Patients. Journal of the Association for Vascular Access. 2010;15(1):16-9.
32. Cope DG, Elledge CM, Thompson Mackey H, Moran AB, Rogers MA, Schulmeister L, et al. Access Device Standards of Practice for Oncology Nursing. Society ON, editor. Pittsburgh, Pennsylvania: Oncology Nurses Society.; 2017.
33. Johnson ND, Minano G. Upper Limb PICC Tip Guideline. In: Centre CCsHM, editor. 2020.
34. Gorski L, Hadaway L, Hagle ME, McGoldrick M, Orr M, Doellman D. Infusion therapy: standards of practice. Journal of Infusion Nursing. 2016;39(1S):S1-S159.
35. Gorski LA, Hadaway L, Hagle ME, Broadhurst D, Clare S, Kleidon T, et al. Infusion Therapy Standards of Practice, 8th Edition. Journal of Infusion Nursing. 2021;44(1S).
36. Bonciarelli G, Batacchi S, Biffi R, Buononato M, Damascelli B, Ghibaudo F, et al. GAVeCeLT consensus statement on the correct use of totally implantable venous access devices for diagnostic radiology procedures. J. 2011;12(4):292-305.
37. Bradford NK, Edwards RM, Chan RJ. Heparin versus 0.9% sodium chloride intermittent flushing for the prevention of occlusion in long term central venous catheters in infants and children. Cochrane Database Syst Rev. 2015(11).
38. Szeinbach SL, Pauline J, Villa KF, Commerford SR, Collins A, Seoane-Vazquez E. Evaluating catheter complications and outcomes in patients receiving home parenteral nutrition. Journal of Evaluation in Clinical Practice. 2015;21(1):153-9.
39. Bell DJ, Knipe H. Superior cavoatrial junction 2020 [updated Feb 2020. Available from: https://radiopaedia.org/articles/superior-cavoatrial-junction-1.
40. Almasi-Sperling V, Hieber S, Lermann J, Strahl O, Beckmann MW, Lang W, et al. Femoral Placement of Totally Implantable Venous Access Ports in Patients with Bilateral Breast Cancer. . Geburtshilfe und Frauenheilkunde 2016;76(1):53-8.
41. Pittiruti M. A new trend in venous access programs: PICC first: slideshare; 2012 [Available from: https://www.slideshare.net/PAIRSPanArabInterven/tarting-your-venous-access-program.
42. Revel-Vilk S, Yacobovich J, Tamary H, Goldstein G, Nemet S, Weintraub M, et al. Risk factors for central venous catheter thrombotic complications in children and adolescents with cancer. Cancer. 2010(Jun 8).
43. Redkar R, Bangar A, Krishnan J, Raj V, Swathi C, Joshi S. Role of Chemoports in Children with Hematological/Solid Tumor Malignancies - Technical Implications and Complications: An Institutional Experience. J Indian Assoc Pediatr Surg. 2019;24(1):27-30.
44. Solinas G, Platini F, Trivellato M, Rigo C, Alabiso O, Galetto AS. Port in oncology practice: 3-monthly locking with normal saline for catheter maintenance, a preliminary report. J. 2017;18(4):325-7.
45. Buchini S, Scarsini S, Montico M, Buzzetti R, Ronfani L, Decorti C. Management of central venous catheters in pediatric onco-hematology using 0.9% sodium chloride and positive-pressure-valve needleless connector. Eur J Oncol Nurs. 2014;18(4):393-6.
46. Tsao K, Fuller CL, Green HL, Jacquez RA, Jackson AA, Andrassy RJ, et al. Risk factors and treatment of port thrombosis in pediatric oncology patients. J Surg Res. 2010;158(2):367-8.